1042
Views & Citations42
Likes & Shares
Introduction:
Vaginal discharge syndrome is an infectious process of the vagina with a florid
symptomatology and psychosocial impact on the female population. Objective: To
characterize the patients of childbearing age with vaginal discharge syndrome
in the Basic Working Group number 2 of the Párraga polyclinic between January
and December 2018.
Method:
Observational, descriptive and cross-sectional study. 195 patients of
childbearing age (between 15 and 49 years of age) of the medical office 10 were
studied in the period from January to December 2018 who attended the medical
consultation referring to presenting vaginal discharge and/or associated
symptoms performing anamnesis, physical examination and microbiological study.
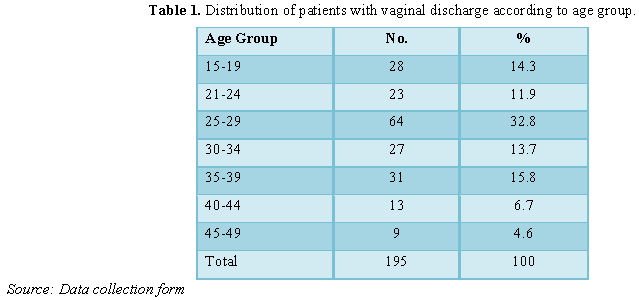
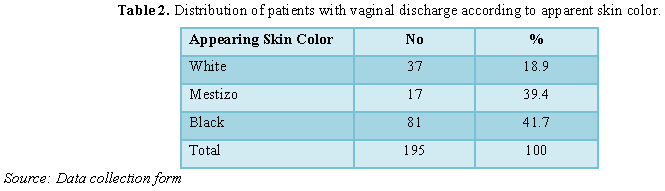
Results: 32.8% were between 25 and 29 years old and
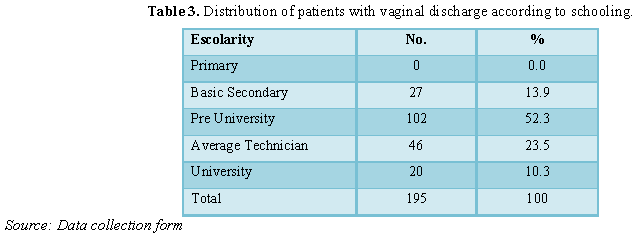
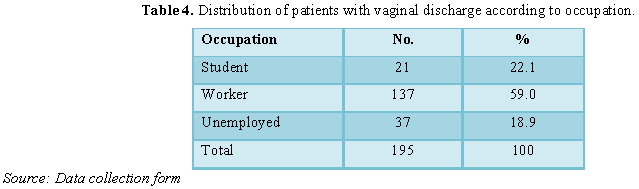
41.7% were black. At least half were 52.3% pre-university; more than 59.0% were
workers. The majority began sexual intercourse before the age of 20. 90.3%
presented risk factors associated with vaginal discharge. The white, lumpy
caseous flow represented 63.1%. At least 9 out of 10 patients presented
vaginitis. More than 75% had Monilia or Gardnerella vaginalis. It was found
that 95% of patients with vaginitis had risk factors.
Conclusion:
Patients predominated between the second and third decade of life of the black
race, with the pre-university concluded and workers. The majority were single
or accompanied, had begun their sexual life at an early age and presented risk
factors. Patients with vaginitis prevailed, with white, lumpy, case-like
discharge and with Monilia as the germ causing vaginal discharge. There was a
statistically significant relationship between the presence of risk factors and
the flow classification.
Keywords:
Vaginal discharge syndrome, Risk factor, Sexual risk
behavior
INTRODUCTION
Vaginal discharge is a common reason for
gynecological consultation at any age, being highly frequent in women of
childbearing age, who are concerned about their reproductive health [1].
Vaginal discharge syndrome is an infectious process of the vagina characterized
by one or more of the following symptoms: leucorrhoea, vulvar pruritus,
burning, irritation, dysuria, dyspareunia, vaginal fetus, determined by the
invasion and multiplication of any microorganism and as a result of an
environmental imbalance in the vaginal ecosystem [2]. This pathology has a wide
range of causal germs and is easy to diagnose and its complications are
frequently related to infantile and reproductive maternal morbidity [2,3]. They
continue to be a public health problem in the world, they are more frequent in
young, single adults and in urban areas, but without anyone with active sex
life being exempt from suffering them. They can also cause complications or
sequelae in both women and men and children, for example orchiepidimitis, acute
pelvic inflammatory disease (herein after EIPA), sterility in both sexes,
penile or cervix cancer, pregnancy complications, miscarriages, death fetal
and/or maternal, premature birth, low birth weight, neonatal infections,
congenital malformations and at risk of transmitting or becoming infected by
the human immunodeficiency virus (here in after HIV) as demonstrated by several
studies [4-7]. In medical practice, vaginal infections
represent a frequent health
Syndromic management represents an alternative to
efficiently address this problem and with this type of approach the treatment
of the causes most frequently associated with the syndrome in question is
achieved and therefore the solution of more than 95% of cases is guaranteed
[9].
The World Health Organization (WHO) estimated
that 333 million new cases of curable sexually transmitted diseases annually in
people aged 15 to 49, mostly in developing countries, which include member
countries of the European community. On the other hand, recent calculations
report that each year more than 340 million Cases of curable Sexually
Transmitted Infections (STIs) (including only those fungal and parasitic
bacterial infections), which have as a manifestation the vaginal discharge
syndrome, susceptible to effective treatments and that at least one million
infections occur every day. For Latin America and the Caribbean alone, between
35 and 40 million cases of this group of Sexually Transmitted Infection were
infected with more than 100 thousand infections per day [4,5]. Vaginal
candidiasis is caused by a fungus or yeast found in the vulvo-vaginal mucosa
that proliferates favored by broad-spectrum antibiotics, oral contraceptives,
pregnancy, menstruation, diabetes mellitus, tight clothing, HIV infection, poor
hygiene habits, etc. Women usually present with vulvar irritation and scarce
exudate. The vulva may appear inflamed with excoriations and fissures. The
vaginal wall may be covered by white, sticky and sticky yeast colonies. This
entity began to be considered as a sexually transmitted infection as of 1967
and it is currently accepted that 50% of the reported cases are the product of
sexual contact. Its treatment consists in the use of clotrimazole 100 mg,
intravaginal twice a day for 3 days or nystatin 100 000 U (vaginal ovum)
intravaginally, once a day for 14 days [10]. In primary health care services
these infections in adolescents are among the first causes of consultation,
with a much higher incidence in those young people with active sexual life,
although they have also been found in virgin adolescents (eleven). Vaginal
symptoms are the most frequent reason for gynecology, being responsible for 6
to 10 million medical visits a year in the world [7]. In the United States
about 30% of women of reproductive age have Bacterial Vaginosis (BV). Almost
75% of all adult women have had at least one fungal infection in their lives.
About 3% of women of reproductive age have trichomoniasis. Many women with
vaginal infections have no symptoms, for example, only 16% of women with
bacterial vaginosis report having vaginal symptoms, while out of every 100
women who have symptoms, such as pain, itching and discharge; 40 to 45 women
have bacterial vaginitis; 20 to 25 women have a fungal infection; 15 to 20
women have trichomoniasis [7-12]. The World Health Organization reported that
since 2006 approximately 15,700 women annually go to vaginal health problems in
primary care facilities in West African countries (Ghana, Guinea, Mali and
Togo), with very low cure rates associated with the costs and non-compliances
of the treatment [7]. The results in European countries are also relevant with
an estimated 250,000 women who, of childbearing age, go annually to vaginal
discharge consultations. Being the most significant figure in women during
pregnancy [7]. In Colombia, the prevalence in Colombia of bacterial vaginosis
has varied between 9% in asymptomatic pregnant women and 30% in non-pregnant
women from the general population [8]. Cuba does not escape this situation,
reporting 831787 consultations by these entities [7-12] Havana reports in 2017;
627 251 patients assessed by obstetrics consultation, while gynecology attended
208,589 women of childbearing age, if we take into account that approximately
75% of the consultations are due to vaginal discharge, the total number of
patients treated is 156 441 [13]. In the Municipality, 19407 patients treated
for vaginal infections in the analyzed period are reported [14]. Regarding the
Párraga Polyclinic, they behave with 4317 patients assisted in gynecology due
to this identity [15].
METHODS
A descriptive
and cross-sectional observational study was carried out. 195 patients of
childbearing age (between 15 and 49 years of age) of the medical office 10 were
studied in the period from January to December 2018 who attended the medical
consultation referring to presenting vaginal discharge and/or associated
symptoms performing anamnesis, physical examination and microbiological study.
Inclusion and exclusion criteria
Inclusion criteria: Female
patients of childbearing age with vaginal discharge who agreed to physical
examination with speculum and attended vaginal and endocervical exudate.
Exclusion criteria: Patients who
do not belong to the health area. Pregnant patients. Patients who have refused
to participate in the investigation.
Technical and procedures
Sources of obtaining the information: Application of a data collection form (Annex 1) to the patients from which the related variables were
studied.
Data registre: A data base
was créate in the Microsoft Office Excel 2010 program where the variables
contained in the Form being investigated were included.
Processing and analysis of information
The variables
included in the Return were entered into a database in Excel and the statistical
processing was carried out in the statistical package Stadistical Package for
Social Science for Personal Computer (SPSS-PC) in its version 19.1 for Windows,
from which it They will prepare tables that summarize quantitative variables in
absolute values and percentages. In addition, statistical tests of independence
χ2 (Chi-Square) will be performed on qualitative variables.
Ethical aspects
The research
was endorsed by the Commission of Medical Ethics in Research of the Faculty of
Medical Sciences “Julio Trigo López”. No new or experimental medications or
techniques were used, which were not yet certified or endorsed for use. No
experimental surgical procedures were performed.
Results
The results in relation to the apparent skin color reflect that the
minority were white 37 cases (18.9%) and there were no significant differences
between mestizo and black (Table 2).
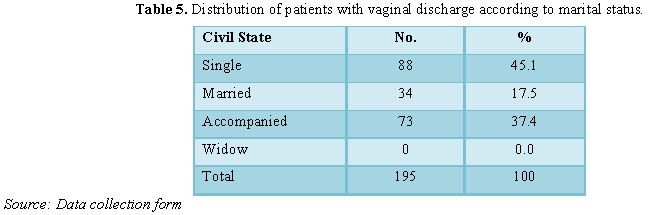
Among the 195 cases studied there were no widows and the majority
corresponded to single women and accompanied with at least 8 out of 10 cases (Table 5).
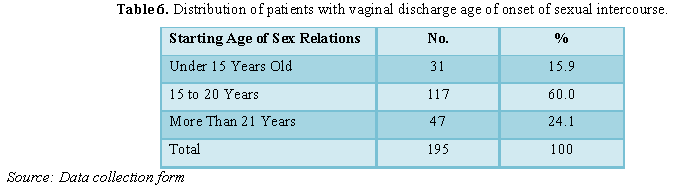
In the study group, 75.9% began their sexual relations before the age of 20
(Table 6).
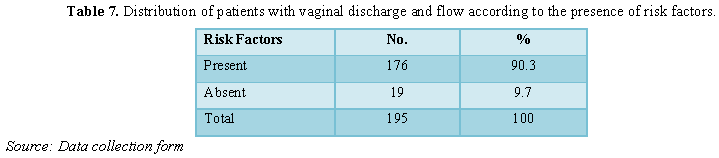
Of the total 9 out of 10 presented risk factors under study (Table 7).
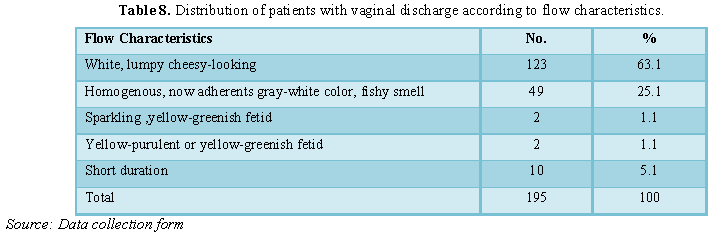
In 6 out of 10
patients, the flow was white, lumpy with a cheesy appearance and in less than
10% yellow-purulent or yellow-greenish, fetid or scarce and short-lived (Table 8).
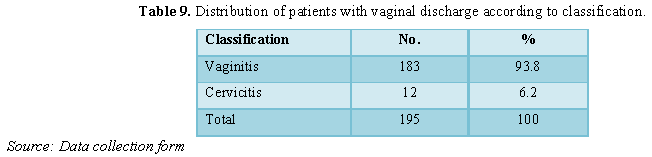
The majority
presented vaginitis 183 patients for 93.8% (Table
9).
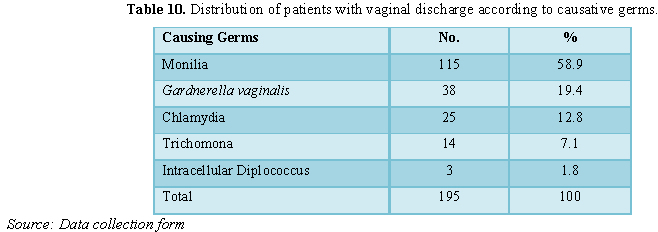
Patients with
Monilia (115; 58.9%) prevailed, followed by those with Gardnerella vaginalis and Chlamydia (38; 19.4 and 25; 12.8
respectively) (Table 10).
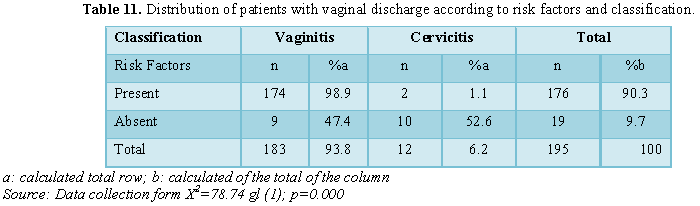
More than 95%
of the patients studied with vaginitis had risk factors. In the absence of
these, more than half had cervicitis. There was a relationship between the
variables risk factors and classification with a significance level of 5% and a
degree of freedom (Table 11).
DISCUSSION
The development of preventive medicine, with the participation of the
doctor and the family nurse, together with the substantial technical and
organizational changes to improve the quality of medical care, have forced us
to look for more dynamic ways that favor the performance of the medical team.
Health, among which is the early detection of vaginal infections [16-18].
Vaginal infections affect women of all ages, both those who are sexually
active, and those who are not. Most of the visits of adult women to
gynecologists and primary care doctors have been more frequent [19,20]. The
results obtained regarding vaginal discharge syndrome and age groups were
comparatively similar to studies carried out in the province and even in the
municipality with a predominance of women between 20 and 30 years of age [9].
In the study by Vidal Borras [16] carried out in Caracas, Venezuela as in the
present, patients between 25 and 29 years predominated and an inversely
proportional relationship between the number of patients affected and the age
as defined above. On the other hand, in the study of Álvarez Blanco et al.
[20], the age of greatest frequency was between 21 and 25 years. The analysis
of the color of the skin and the incidence of vaginal flow syndrome showed a
higher frequency between black and mixed race in that order. Probably related
to the ethnic characteristics of the place where the study population
predominates. No serious studies were found in the literature that address the
issue from this point of view, however, we believe that there could be an influence
determined by particularities of the sexual characteristics of each race, such
as those of black race show a more early and bulky development of secondary
sexual characteristics such as breast, hip or butt growth, being able to
identify with higher stages of sexual development and anticipate sexual
behavior, often at risk. State education, free, equal and compulsory; at least
until the ninth grade, which guarantees a level of instruction and education
comparable even to that of highly developed nations; it is one of the
characteristics of our nation. Therefore, starting in active working life is an
option and not an obligation as it is for adolescents in many countries. A
female student, usually younger, does not have economic independence and
usually has plans to continue her improvement and achieve a job placement
according to her level of qualification. In these circumstances, and taking
into account that the expired institutional educational level was taken into
account, it was not surprising to find a majority of pre-university students,
followed by those with a mid-level technician and a basic secondary school
.This result corresponds to those published by the Alan Gulttmacher Institute
[21] and the United Nations Population Fund [22]; as with Hurtado
Saucedo [23] in his thesis of ‘Specialty in Comprehensive General Medicine’,
also carried out in our health area between 2013 and 2014. In our country the
female population has been increasingly incorporated into schooling and the
aspiration and need to develop some activity of its own, expanding work options
for women. In the present investigation a predominance of the patients linked
to some type of work activity was evidenced, as well as in the aforementioned
study by Hurtado Saucedo [23], however, this series exceeded ours in percentage
terms in terms of the unemployed population. In the study, single and
accompanied women represented the majority, corresponding to published national
results [9,16]. While, the age of onset of sexual intercourse was early in the
majority before the age of 20. Series such as that of Ugarte Rodríguez [24]
with similar results, discuss how the early onset of sexual intercourse
significantly affects the presence of vaginal discharge, because age is a
biological factor that influences the presence of it by the constitution The
vaginal mucosa and cervical tissue of the young woman make them very
susceptible to this entity. Much has been written about the risk factors
associated with vaginal discharge syndrome, which constitutes a huge challenge
to be faced by professionals dedicated to the promotion and prevention of
sexual and reproductive health. In the literature, several articles related
mainly to gravity were found, a subject that although useful, for the purposes
of this research were taken into account, but this group was intentionally
excluded due to the particular characteristics and connotation it has in
primary care this combination; possible subject for future research. It is also
relevant in the reading as the risk factors associated with the presence of
vaginal discharge are often analyzed independently. It was intended to
investigate them, analyze them in terms of their presence or absence because it
offers a more accurate understanding of the phenomenon, taking into account
that a patient sometimes presented more than one risk factor. In our series,
the absence of risk factors represented the minority of cases. These results
correspond to those of Cordero Ruiz [25], published in Argentina and Escobar
Acosta and collaborators published in the Proceedings of the XIII Congress of
the Cuban Society of Obstetrics and Gynecology at the Palacio de Convenciones
[26-28] where Most of the patients presented at least one of the risk factors
analyzed.
Also with
studies published in the area of health in question by Hurtado Saucedo [23] and
Jira Herrera [27] treating these last two thesis studies presented in option to
the specialty of 1st degree in General Medicine Integral. The most
frequent clinical manifestation in the present work was lumpy white with a
cheesy appearance and the most frequent diagnosis was vaginitis [29-32]. While
the predominant microbiological result was the corresponding one with Monilia
followed by Gardnerella vaginalis.
Similar results to several published studies such as that of Puentes Rizo et
al. [9] in ‘Behavior of the Vaginal Syndrome in a Párraga Office’, for whom
this clinical manifestation was the second most frequent. And these germs were,
although in reverse, also the most frequent, coinciding with our study in which
more than 75% presented this etiology. In their study of cervico-vaginal
infections in patients treated in an infertility clinic, Román et al. [28] also
reported as the main clinical manifestations of the homogeneous gray-white
vaginal discharge in 40, 9%, that although it was not the predominant one in
our series, it was similar.
The
association between the presence of risk factors and the classification of
vaginal discharge in vaginitis or cervicitis was highly significant. Observing
that in the absence of these the majority presented cervicitis and its presence
the vaginitis. Among other elements related to the fact that the latter are
more frequent [32-36]. The phenomenon addressed imposes a challenge on Public
Health in Cuba, to improve the quality of life of women of childbearing age and
programs to provide information on the subject must continue to be developed.
CONCLUSION
1.
Humpiri Paredes L
(2018). Síndrome de flujo vaginal. Available at: https://plus.google.com/104834283153123540903
2.
Cires M, Freijoso E,
Silva L, Vergara E, Cutie E, et al. (2014) Guía para la práctica clínica de las
infecciones vaginales. Rev Cubana Farm 37: 38-52.
3.
ACOG (2016) Practice
bulletin. Clinical Management Guidelines for Obstetrician and Gynecologist 72.
4.
Colectivo de autores
(2014) Infecciones de transmisión sexual. Pautas para su tratamiento. La
Habana: Ministerio de Salud de la República de Cuba, pp: 7-48.
5.
Beers MH (2017) El
Manual Merck de diagnóstico y tratamiento. 11na ed. Madrid: Elsevier.
6.
Cutié Bresler M,
Almaguer J, Álvarez M (2015) Vaginosis bacteriana en edades tempranas. Rev
Cubana Obstet Ginecol 25: 174-180.
7.
Sherrard J, Donders G,
White D, Jensen J, Iusti E (2011) European (IUSTI/WHO) guideline on the
management of vaginal discharge. Int J STD AIDS 22.
8.
American Journal of
Obstetrics and Gynecology (2018) Crece la actividad sexual en adolescentes y
decrece el uso del condón.
9.
Puentes Rizo EM,
Enríquez Domínguez B, Jiménez Chacón MC, López Rodríguez P (2009)
Comportamiento del síndrome de flujo vaginal en el consultorio 16, Policlínico
Párraga. Rev Cubana Obstet Ginecol 35.
10.
Harter P, Sehouli J,
Lorusso D, Reuss A, Vergote I, et al. (2017) A randomized trial of
lymphadenectomy in patients with advanced ovarian neoplasms. N Eng J Med 380:
822-832.
11.
Faro S, Martens M,
Maccato M, Hammill H, Pearlman M (2014) Vaginal flora and pelvic inflammatory
disease. Am J Obstet Gynecol 169: 470-474.
12.
Fernández Limia O,
Betancourt A, Lesteiro M (2015) Prevalencia por diagnóstico inmunológico de Candida spp., Trichomonas vaginalis y Gardnerella
vaginalis en mujeres embarazadas a nivel primario del sistema de salud. Rev
Cubana Obstet Ginecol 36.
13.
Anuario Estadístico De
Salud (2017) ISSN Versión electrónica 15.62-4433. Ministerio de Salud Publica
.Dirección de registros médicos y estadísticas de salud. La Habana 2018.
14.
Hamilton G, Falistocco
C (2017) Guía de Manejo de las Infecciones de Transmisión Sexual. Rep
Argentina.
15.
CDC (2014) Guidelines
for treatment of sexually transmitted diseases. Guidelines for Management of
Sexually Transmitted Infections of the World Health.
16.
Vidal Borras E (2016)
Síndrome de flujo vaginal. Revista Cubana de Obstetricia y Ginecología 36:
594-602.
17.
CDC staff members
(2018) Center for disease control and prevention. 2018 Guidelines for treatment
of sexually transmitted diseases. MMWR 47: 70-79.
18.
Biswas MK (2014)
Vaginosis bacteriana. Clínicas Obstétricas y Ginecológicas 1: 165-174.
19.
Mc Coy MC, Katz VL, Kuller JA, Killam AP,
Livengood CH (2015) Bacterial vaginosis in pregnancy: An approach for the
1990s. Obstet Gynecol Survey 50: 482-488.
20.
Alvarez Blanco DA
(2014) Comportamiento del Síndrome de Flujo Vaginal. Policlínico Darío
Calzadilla Angulo. Enero a Julio.
21.
FNUAP (2016) Nueva
campaña contra el embarazo en la adolescencia. POPULI la revista de la FNUAP
28: 3.
22.
Fondo de las Naciones
Unidas para la Infancia (2016) La Adolescencia una época de oportunidades.
Estado Mundial de la Infancia 2016. UNICEF.
23.
Hurtado Saucedo PM
(2014) Caracterización del Síndrome de Flujo Vaginal en el CMF # 30.
Policlínico Párraga. Arroyo Naranjo. La Habana. 2013-2014. Tesis de terminación
de especialidad en Medicina General Integral.
24.
Ugarte Rodríguez CJ
(2007) Prevalencia de infecciones cervico-vaginales en embarazadas en un
hospital obstétrico de referencia de Ciudad de la Habana. Rev Cubana Obstet
Ginecol 33: 2.
25.
Cordero Ruiz DM, Silva
García K, Fuste Pedroso W, Rey Sánchez ML, Visconti Marin C (2017) Síndrome de
flujo vaginal: Un problema de salud? Rev Ciencias.com. Argentina: Edit.
Científica.
26.
Escobar Acosta A, Cutié
M (2017) Vaginosis bacteriana en edades tempranas. Actas del XIII Congreso de
la Sociedad Cubana de Obstetricia y Ginecología. Palacio de Convenciones, La
Habana.
27.
Jira Herrera C (2014)
Caractrización Del Síndrome De Flujo Vaginal En El Policlínico Capri. Arroyo
Naranjo La Habana. Año 2013-2014. Tesis de terminación de especialidad en
Medicina General Integral.
28.
Román L, Cervantes M,
León A, Hernández E (2017) Infecciones cérvico-vaginales en pacientes atendidas
en consulta de Infertilidad. Actas del Xlll Congreso de la Sociedad Cubana de
Obstetricia y Ginecología. Palacio de las Convenciones. La Habana.
29.
Currants D, FAGOG MD,
Hansen E, Fellow DO (2016) Gardnerella. Available at: http://www.emedicine.com/obgyn/index.shtm//sexually
30.
CDC (2014) Diseases
characterized by vaginal diseases treatment guidelines. MMWR Recomm Rep 51:
42-48.
31.
Owen MK, ClenneeyTL
(2014) Management of vaginitis. Am Farm Physician 70: 2125-2132.
32.
León J (2014) Tratado
de Obstetricia. Edit. Científica Argentina, Buenos Aires. T III, p: 995.
33.
Cuba, Ministerio de
Salud Pública (2015) Dirección Nacional de Epidemiología. Dirección Materno
Infantil. Programa nacional de prevención y control de ITS/VIH/SIDA. Manejo
sindrómico del flujo vaginal en gestantes [Internet]. La Habana: MINSAP.
34.
Roget M (2015)
Secreciones Vaginales. Una señal en la mujer adulta. Salud. Vid. Available at: http://www.emedicine.com/obgyn/index.shtm/#sexually
35.
Omnia M, Samra MD (2015)
Vulvovaginitis. Medicine Specialties. Obtetrics and Gynecology 2015: 1-10.
36. Jaqulery A, Stylianopoulos A, Hogg G (2014) Vulvovaginitis: Clinical features; etiology and microbiology of the genital tract. Arch Dis Child 81: 64-67.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
-
Table 9
-
Table 10
-
Table 11
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Journal of Alcoholism Clinical Research
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Spine Diseases
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)


